Dr Nitish Jhawar, Head of Colorectal department, Fortis Hiranandani Hospital located in Vashi Navi Mumbai recently participated in a Surgical Workshop Training course on the use of Doppler Ultrasound Proctoscope for carrying out the Doppler-Guided Hemorrhoid Artery Ligation (DGHAL) procedure.
The workshop, which was held at A.M.I head office at the Feldkirch & Bludenz General Hospital in Austria, covered key principles, techniques, and protocols regarding the use of the Proctoscope. It also covered the basics of the disease along with its indications as well as a comparison with other available techniques.
The DGHAL is a relatively new advanced operational technique for evaluating and treating haemorrhoids (piles). This minimally invasive procedure uses ultrasound Doppler to accurately identify the site of the piles and enables the tying of the affected vessels as well as repositioning of the haemorrhoidal lumps. A highly effective method, the treatment involves lesser pain and facilitates faster recovery for patients.
The Proctoscope plays a vital role as it guides the process through the Doppler ultrasound probe which is mounted on this specially designed equipment. Understandably it is important to understand the full range of its features, operations and capabilities.
The workshop attended by Dr Jhawar was focused on enabling participants to gain complete knowledge of the equipment, which would help them to better perform examinations using the Proctoscope and implement effective techniques to carry out the treatment.
Dr. Jhawar thanked Dr. Mathias Sheyer, who is the Chief Surgeon of Bludenz General Hospital and has experience in treating over 2000 cases in last 15 years, and Dr. Gruber Andreas for sharing their expertise.
Commenting on the event, Dr Nitish Jhawar said,” It has been an extremely educative experience to attend this workshop. The high rate of success and superior benefits to patients through innovative DGHAL technique makes it an important treatment option, and I will use the knowledge and skill gained from attending this workshop to offer this treatment to my patients.”
Dr. Jhawar is a highly experienced expert in the field of Laparoscopic & Colorectal surgeries. He has previously undergone advanced training in treating piles & Fistula.
He has additionally been trained in VAAFT – Video Assisted Anal Fistula Technique in a session held in Berlin, Germany which included a meeting with Dr. Monreio the inventor of the technique. This endoscopic treatment method offers diagnoses and removal of anal fistulas through fistuloscopy, which avoids surgical excision of the sphincter, making it less painful.
About Dr. Nitish Jhawar
By gaining a deep understanding of the various new and advanced therapies for treating piles, Dr. Jhawar is well placed in offering patients the latest in treatment options for colorectal surgeries. Minimal invasive Endoscopic surgeries are safer, less painful and ensure faster recovery making them the preferred method for many. A wide range of treatments for piles including DGHAL and stapling is available for patients looking for relief from this painful condition.
Dr. Nitish Jhawar General, Laparoscopic and Colorectal Surgeon at Fortis Hiranandani Hospital, Navi Mumbai, India recently attended a surgical workshop at Berlin (Germany )to understand and perform VAAFT – Video Assisted Anal Fistula Technique- better. This endoscopic treatment of fistula doesn’t have a risk of incontinence.
In today’s era of minimally invasive surgeries, emphasis on painless treatment and faster recovery without much dissection of the tissue is higher. Anal fistulas have been treated from the era of Hippocrates from 1600 DC. Everything starting from horse’s hair to laser has been tried to treat these nagging problem. The two main factors / fear in fistula surgery is recurrence and incontinence due to incomplete removal or excessive cutting of sphincter.
There are various surgical ways to treat fistula including removal of the fistula track completely. This is surely painful, requires daily dressing and also takes a lot of time to heal. Along with which there are higher chances of recurrence; whereas, VAAFT requires no incision, which helps patients to resume their daily lives with ease.
This endoscopic treatment offers a complete diagnosis of the fistulous tract in the form of fistuloscopy and since no cutting of the sphincter is involved, there is no risk of incontinence. The latest case studies are showing encouraging results in this particular modality. Tackling recurrence of the fistula with VAAFT is much easier option and acceptable to the patient because of its painless patient-friendly treatment.
On his visit to Berlin, Dr. Nitish Jhawar met Dr. Monreio, who is the inventor of this technique and have more than 10 centres all over the world.
Dr. Monreio takes pride in the efficacy of this treatment which is helping him treat patients all across the Globe. As per Dr. Jhawar –“ It was a wonderful experience to learn the Nitti gritty of the surgical challenges and their management from the inventor himself. VAAFT has clearly achieved a reputed place in ARMAMENTARIUM of fistula treatment modalities and is here to stay. I am aiming to continue his legacy of helping people with VAAFT and make it easier for the patients suffering from Anal Fistula.”
The stomach normally secretes acid that is essential in the digestive process. This acid helps in breaking down the food during digestion. When there is excess production of acid by the gastric glands of the stomach, it results in the condition known as acidity, dyspepsia, heartburn.
Heartburn is burning sensation in mid chest or throat that’s caused by digestive juice acid rising up from stomach to the food pipe or esophagus It’s a common symptom of the condition called gastroesophageal reflux disease or GERD, also called acid reflux or acid regurgitation. Occasional reflux is common , reflux more than twice a week is GERD.
Symptoms:
Heartburn. Most likely to occur in connection with the following activities:
Eating a heavy meal
Bending over
Lifting
Lying down, particularly on the back
Dyspepsia.
Pain and discomfort in the upper abdomen
A feeling of fullness in the stomach
Nausea after eating
Regurgitation. feeling of acid backing up in the throat. Sometimes acid regurgitates as far as the mouth and can be experienced as a “wet burp.”
Less Common Symptoms
Elderly patients with GERD often have less typical symptoms than do younger people. Most children under 12 years with GERD, and some adults, may have GERD without heartburn. Instead, they may have dry cough, asthma symptoms, or trouble swallowing
Chest pain-
Chest pain is a common symptom of GERD. It is very important to differentiate it from chest pain caused by heart conditions.
Symptoms in the Throat-
Acid laryngitis. A condition that includes hoarseness, dry cough, the sensation of having a lump in the throat, and the need to repeatedly clear the throat.
Trouble swallowing. In severe cases, patients may choke or food may become trapped in the esophagus, causing severe chest pain. This may indicate a temporary spasm that narrows the tube, or it could indicate serious esophageal damage or abnormalities.
Chronic sore throat
Persistent hiccups
Coughing and Respiratory Symptoms. Airway symptoms, such as coughing and wheezing, may occur.
Chronic Nausea and Vomiting. Nausea or in rare cases vomiting can occur.
What causes GERD?
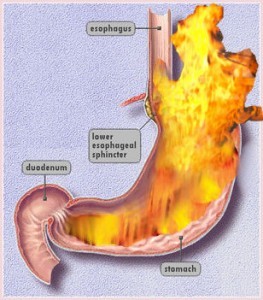
When we eat, food travels from mouth to stomach through a tube called the gullet or esophagus. At the lower end of the esophagus is a small ring of muscle called the lower esophageal sphincter (LES) which acts like a one-way valve, allowing food to pass through into the stomach. Normally, it prevent back-flow of stomach juices (acid)) into the esophagus. GERD occurs when the LES does not function properly allowing acid to flow back and burn the lower esophagus. This irritates and inflames the esophagus, causing heartburn and eventually may damage the esophagus. Research shows that in people with GERD, the LES relaxes while the rest of the esophagus is working. There may be Impaired Stomach Function or Motility Abnormalities.About 30 – 40% of reflux may be hereditary.
What contributes to GERD?
Common foods that can worsen reflux symptoms include
citrus fruits
chocolate
Soda
drinks with caffeine or alcohol
fatty and fried foods
garlic and onions
mint flavorings
spicy foods
Tomato
Many other factors can also play a role in triggering heartburn and causing GERD
Overeating. Stomach remains distended when there are large quantities of food in it. The more your stomach stays distended, the more likely the LES won’t close properly. When it doesn’t close, it can’t prevent food and stomach juices from rising back up into the esophagus.
Eating habits. Eating too rapidly, eating while lying down or too close to bed time can be a heartburn trigger.
Smoking. Smoking cigarettes is another potential cause of heartburn.
Hiatal hernia. Your diaphragm is a muscular wall that separates your stomach from your chest. It helps the LES keep stomach acid where it belongs. When the LES and the upper part of the stomach move above the diaphragm you develop a hiatal hernia. The hernia makes acid reflux, which causes heartburn, more likely.
Obesity or overweight. Research suggests that being obese or overweight can be a trigger for heartburn and reflux disease.
Pregnancy. Pregnant women are particularly vulnerable to GERD in their third trimester, as the growing uterus puts increasing pressure on the stomach. Heartburn in such cases is often resistant to dietary interventions and even to antacids.
Medicines. Common medications taken for other problems can increase the likelihood of heartburn. That includes medicines used to treat asthma, high blood pressure, heart problems, arthritis or other inflammation, osteoporosis, anxiety, insomnia, depression, pain, Parkinson’s disease, muscle spasm, or cancer.
Exercise. Increased pressure on the abdomen can increase the risk of acid reflux. Weightlifters had the most heartburn and acid reflux. Runners had milder symptoms and less reflux than weightlifters.
How is GERD treated?
If you have had symptoms of GERD and have been using antacids or other over-the-counter reflux medications for more than 2 weeks visit a gastroenterologist
Depending on the severity of your GERD, treatment may involve one or more of the following lifestyle changes, medications, or surgery.
General Measures – Self-Care
Some dietary and lifestyle tips for heartburn relief-
Avoid trigger foods. Classic GERD triggers include chocolate, coffee, cols, alcohol, peppermint, citrus juices, and tomatoes. The exact food triggers vary from person to person
Don’t eat before bed. You shouldn’t eat two to three hours before bed. Not eating gives your stomach time to empty before you lie down.
Loosen your belt. Tight belts or pants can aggravate your GERD symptoms. Wear looser clothing, especially at night.
Prop up the bed. When you stick blocks under the head of your bed and raise it 6 to 8 inches, gravity will prevent the acids in your stomach from flowing into the esophagus during the night.
Lose weight. If you’re obese, aiming for a 10% weight loss is always a good idea.
Evaluate your other medications. Many common medications — aspirin and other NSAID painkillers, along with some drugs for high blood pressure — can make GERD worse.
Stop smoking.
Medications for GERD
Antacids, are usually the first drugs recommended to relieve heartburn and other mild GERD symptoms.
Foaming agents, work by covering your stomach contents with foam to prevent reflux.
H2 blockers, ranitidine decrease acid production. provide short-term relief and are effective.
Proton pump inhibitors omeprazole lansoprazole pantoprazole , rabeprazole and esomeprazole are more effective than H2 blockers and can relieve symptoms and heal the esophageal lining.
Prokinetics help strengthen the LES and make the stomach empty faster. This group includes bethanechol (Urecholine) and metoclopramide (Reglan). Metoclopramide also improves muscle action in the digestive tract. Prokinetics have frequent side effects that limit their usefulness—fatigue, sleepiness, depression, anxiety,
What if GERD symptoms persist?
If your symptoms do not improve with lifestyle changes or medications, you may need additional tests.
Barium swallow radiograph uses x rays to help spot abnormalities such as a hiatal hernia and other structural or anatomical problems of the esophagus. With this test, you drink a solution and then x rays are taken. The test will not detect mild irritation, although strictures—narrowing of the esophagus—and ulcers can be observed.
Upper endoscopy is more accurate than a barium swallow radiograph. The doctor may spray your throat to numb it and then, will slide a thin, flexible plastic tube with a light and lens on the end called an endoscope down your throat. The endoscope allows the doctor to see the surface of the esophagus and search for abnormalities.
The doctor also may perform a biopsy. The tissue is then viewed with a microscope to look for damage caused by acid reflux and to rule out other problems if infection or abnormal growths are not found.
pH monitoring examination through a small tube into the esophagus or a tiny device to the esophagus that will stay there for 24 to 48 hours. when and how much acid comes up into your esophagus is measured. This test can be useful if combined with a carefully completed diary—recording when, what, and amounts the person eats—which allows the doctor to see correlations between symptoms and reflux episodes.
Surgery For GERD
Surgery is an option when medicine and lifestyle changes do not help to manage GERD symptoms. Surgery may also be a reasonable alternative to a lifetime of drugs and discomfort. With the new minimally invasive approach, surgery is now a viable initial therapy and is safe and effective in people of all ages, including infants.
Nissen Fundoplication is surgery to repair hiatal hernia and is surgical treatment for GERD. Upper part of the stomach is wrapped around the LES to strengthen the sphincter, prevent acid reflux, and repair a hiatal hernia.
Endoscopic techniques. In one endoscopic method for treating GERD, an instrument is inserted that delivers an electrical current to the lower esophageal sphincter. This results in scarring which tightens the sphincter. In a second method, sutures are placed in the sphincter to tighten the sphincter
What are the long-term complications of GERD?
Having heartburn more than occasionally can reduce your quality of life. It can affect not just what you eat, but how you sleep and what activities you do.
Chronic GERD that is untreated can cause serious complications. Inflammation of the esophagus from refluxed stomach acid can damage the lining and cause bleeding or ulcers—also called esophagitis. Scars from tissue damage can lead to strictures—narrowing of the esophagus—that make swallowing difficult.
Some people develop Barrett’s esophagus, in which cells in the esophageal lining take on an abnormal shape and color. Over time, the cells can lead to esophageal cancer, which is often fatal.
Studies have shown that GERD may worsen or contribute to asthma, chronic cough, and pulmonary fibrosis.
1Q. I am a 25 yr old sportsman. I noticed a lump in my groin 3 days ago. My family physician diagnosed it as hernia & advised surgical opinion want to know what a Hernia is?
A. Hernia is a protrusion of contents of the abdomen through a weakness or tear in its muscles forming a lump underneath the skin. Mostly it is seen in groin but it may be present on abdominal wall above, at or below umbilicus & at the site of surgical scars.
2Q. I have a Hernia near my naval but it is painless, soft & disappears on lying down, very rarely it swells turgid or pains. Do I still have to go for surgery?
A. Most of the Hernias, irrespective of the site, are painless to start with. The main symptom is a bulge which comes on straining and disappears on lying down. As the treatment of hernia is surgical it is better to undergo surgery when it is uncomplicated. The possible complications include obstruction or strangulation which may be life threatening.
3Q. Is surgery a must for a Hernia and what are the options which I can choose from?
A. Depending on the type & location of Hernia, your surgeon will decide the type of repair. On a broader spectrum we can understand that Hernias can be repaired by open surgical method or by Minimal access surgery (keyhole surgery). Modern surgical practices use reinforcement in the form of polypropolene meshes. In our hospital we prefer, to perform minimal or laproscopic surgery for all our patients if they are fit to tolerate general anaesthesia.
4Q. How long it will take to recover after Hernia surgery?
A. Depending on the type of repair, the period varies from3-5 days. In laproscopic surgery, it is much faster and in open cases it may take little longer.
5Q. When can I return to work after surgery?
A. If you have a desk job, 3-5 days is the time frame we are looking at. But if your job demands heavy physical activity like lifting weight and all – you are away from work for 4 to 6 weeks.
6Q. I have a Hernia surgery planned next week. Can I drive back home after discharge?
A. We usually advise our patients to abstain from driving for 48hrs till the effect of anaesthesia subsides & their movements become comfortable.
7Q. Can my Hernia be repaired using single incision laparoscopy?
A. Depending on the size of Hernia and fitness of the patient SILS can be offered. We prefer SILS using Single port multiple incision technique.
8Q. I delivered my 2nd baby an year ago and noticed a lump by the side of previous surgery scar. Doctor suggested repair using a mesh. I am scared to have a foreign body inside what to do?
A. It is now a common practice to use meshes which are made of synthetic materials like polypropelene or polyester to reinforce the Hernia repair. Person who is having Hernia has a inherent defect in cementing substance called collagen, mesh provides a lattice for body fibres to grow in between & render a stronger repair. As the meshes are biologically inert, they are harmless if left in body for good.
9Q. My father was operated for Hernia long back. Do I need to undergo checkup to rule out the same? Is hernia hereditary?
A. You may have more chances of developing Hernia than normal population but it is not hereditary. Factors which are causing intra-abdominal strains like pregnancy, obesity, coughing, urinary obstructions may all lead to Hernia if there is a weakness in the wall. Some Hernias may be present from birth & are called Congenital Hernias.
10Q. My mother is 55yrs old & she has been operated for Ventral Hernia twice but it has recurred. She has a 12cm defect in the midline. What kind of repair will solve her problem?
A. Old age, obesity and hereditary predisposition causes Hernias to recur. In your case latest surgical technique of Component Separation should do the trick. In this type of repair, we mobilize the muscles of the abdominal wall in such a way that we can achieve closure in the midline using normal muscles & sheath and reinforce the same by use of meshes. This technique is a boon for people having large defects, recurrent Hernias & is gaining popularity worldwide.
11Q. I have noticed that my belly button becomes prominent on standing & coughing. I have read on internet & it looks like Hernia. What tests should I do to confirm my diagnosis?
A. Mostly Hernias are diagnosed on clinical examination & do not require any sophisticated investigations to confirm the diagnosis. We may get some help by doing tests like sonography, CT scan and MRI of the abdomen. Though they are mandatory in complicated, obstructed and recurrent cases, they are not usually required in uncomplicated cases like yours.
There is no sure evidence to prevent Gallstones but it is possible to have an effective gallstone diet plan to reduce risk. Research has also shown that Vegetarians have a significantly lower risk of developing gallstones, compared to people who eat meat.
Gallstones are pieces of solid material that form in the gallbladder, a small organ located under the liver. These stones develop because cholesterol and pigments in bile sometimes form hard particles. Read More about Gall Bladder stone at neoalta.com
Two main types of gallstones are:
Cholesterol stones: Usually yellow-green in color, approximately 80% of gallstones are cholesterol stones.
Pigment stones: These stones are smaller and darker and are made up of bilirubin.
Causes of Gallstones
Genetics – If other people in your family have had gallstones, you are at increased risk of developing gallstones.
Obesity – This is one of the biggest risk factors. Obesity can cause a rise in cholesterol and can also keep the gallbladder from emptying completely.
Estrogen – Estrogen can increase cholesterol and reduce gallbladder motility. Women who are pregnant or who take birth control pills or hormone replacement therapy have higher levels of estrogen and may be more likely to develop gallstones.
Ethnic background – Certain ethnic groups, including Native Americans and Mexican-Americans, are more likely to develop gallstones.
Gender & Age – Gallstones are more common among women and older people.
Cholesterol drugs – Some cholesterol-lowering drugs increase the amount of cholesterol in bile, which may increase the chances of developing cholesterol stones.
Diabetes – People with diabetes tend to have higher levels of triglycerides (a type of blood fat), which is a risk factor for gallstones.
Rapid weight loss –If a person loses weight too quickly, his or her liver secretes extra cholesterol, which may lead to gallstones. Also, fasting may cause the gallbladder to contract less.
Symptoms of gallstones:
A majority of the people may not experience any symptoms. Its your doctor who may find stones in your gallbladder while doing X-rays, ultrasound or surgery in the abdomen. Gallstones most frequently make their presence known when they become lodged in one of the ducts that carry bile, a digestive juice, from the liver to the small intestine and when such an obstruction occurs,the following symptoms might be experienced:
Severe and sudden pain in the upper right abdomen and possibly extending to the upper back
Fever and shivering
Severe nausea and vomiting
Jaundice (yellowing of the skin or eyes)
Clay colored stools or dark urine
How Are Gallstones Diagnosed?
Physical examination that includes checking your eyes and skin for visible changes in color. A yellowish tint in your skin or eyes may be signs of jaundice. The examination may also involve using diagnostic testing to see inside your body. These tests include:
Abdominal CT Scan-This is an imaging test that takes pictures of your liver and abdominal region.
Ultrasound-Ultrasound tests produce images of your abdomen.
Gallbladder Radionuclide Scan-This very important scan takes about one hour to complete. A specialist injects a radioactive substance into your veins. The substance travels through your blood to the liver and gallbladder. It highlights any infection or blockages in these organs.
Blood Tests-Your doctor may order blood tests that measure the amount of bilirubin in your blood. The tests also gauge how well your liver is functioning.
How Are Gallstones Treated?
The most common ways of gallstone treatment are-
Surgeries -Surgery is often the first option if you have symptoms. A surgeon may perform a commonly used technique called laparoscopic gallbladder removal.
Medications -Drugs that dissolve gallstones caused by cholesterol are an option if you cannot undergo surgery. These medications may take several years to eliminate the gallstones.
How can you prevent gallstones?
Certain factors that increase the risk of developing gallstones, such as age, sex and ethnic origin cannot be altered.
But it is possible for us to have a effective gall stone diet plan – low in fat and high in fruit and vegetables, including plenty of dietary fiber, as many experts say that such type of a diet will help protect people from developing gallstones.
Avoid processed food such as read meat, sausages, also French fries , pastire.
Controlling your body weight – not allowing yourself to become overweight/obese – may also help prevent the formation of gallstones.
However, crash dieting and rapid weight loss are risk factors in the development of gallstones so try losing weight gradually following a healthy diet for which you could visit a diet counselor.
A Diet is when you watch what you eat and wish you could eat what you watch.
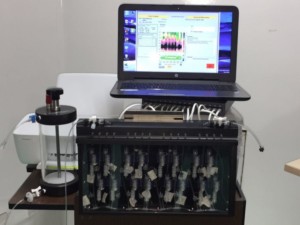
Bringing in a higher level of quality in medical care, Dr Nitish Jhawar who is the Head of Colorectal department at the Fortis Hiranandani hospital located in Vashi Navi Mumbai has introduced a manometry machine to his department.
This will be the first manometry machine available in the whole of Navi Mumbai region.
Manometry tests are key physiological tests that enable doctors to study the Colorectal and Esophageal region. Physiological tests are important because they allow doctors to directly examine how the interior muscles and reflexes are working.
Using Colonic manometry and anorectal manometry doctors are able to understand the pressure and motor activity including sensations and reflexes inside the colon and the anus /rectal region, as well as the strength of the muscles there.
Speaking on the occasion, Dr. Jhawar said,” I am happy to announce that our department will now be able to provide the best in medical investigation for colorectal conditions. The manometry machine plays a vital role in providing information to doctors to diagnose accurately and quickly enabling patients to benefit from the right therapy.”
The test is an important step while evaluating a patient in cases of constipation, stool leakage, or severe abdominal pain which are not responding to other medical therapy and it also helps in deciding whether patient is a candidate for STARR surgery for constipation . Manometry tests often are able to spot issues which are missed by other diagnostic tests like radiology and endoscopy.
The Manometry test is an outpatient procedure, taking only around 30-90 minutes but can be higher in rare cases. Under the procedure a thin flexible tube is inserted into the rectum and the machine then measures the muscle contractions, movement and pressure occurring internally. Patients might need to carry out certain actions so that the machine can record the responses to these manoeuvres.
Completely safe and painless, the test delivers critical inputs to doctors. The results, which are seen in form of graphs, enable medical practitioners to understand the efficacy of motor functions of the affected muscles helping them identify the cause accurately, guiding the doctor in choosing and administering in the correct treatment therapy.
About Dr Nitish Jhawar
Dr Nitish Jhawar is asenior laparoscopic surgeon & Colorectal Surgeon (Colo- Proctologist) at Fortis Hiranandani Hospital Vashi and Neoalta specialty clinic, Vashi, Navi Mumbai. He has received training from Germany and Austria and has over 16 years experience in treating piles, constipation, Anal fistulas and pilonidal sinus through minimally invasive procedures.
Treatments he does include painless piles surgery through techniques such as DGHAL / Stapler, Constipation surgery STARR ,and advanced treatment for fistula such as VAAFT, LASIT , LIFT and LASER.
He also specialises in Laparoscopic Surgery including gall bladder, hernia, appendectomy, and other general surgeries such as diabetic foot, and varicose veins.
I was diagnosed with gall stones a year ago in Delhi, I showed it to a doctor at Max hospital, he just asked me to get a surgery done and get my gall removed on any date of my choice, I was sacred and too young to get it done I got a vibe from doctor that for him it’s just a small things, however according to for a patient it’s important first be convinced on the urgency to get it done and feel safe . A year later I shifted to Mumbai and started having a frequent pain in shoulder blades and gall area. It went sharp this time. We went to Dr Nitish , as oppose to Delhi doc, Dr Nitish was very polite, first asked us to get the scan done and understand the current scenario, the scan showed one big 17 mm stone which was earlier also there but this time also there were multiple various sized stones as well along with the big one. Dr Nitish examined the scan, explained me and my husband about the condition and need of surgery or else the stone Would have slipped in the panacea or bile calling for a bigger operation. He explained diagramatically . He was patient in explaining, gave us time to think and be convinced. We were ready and then he performed it . It was flawless, quick and went well. He is a very experienced and fine surgeon , he is caring and doesn’t create panic at all rather he takes it slowly and makes patient comfortable. It was lapro, it’s been 2 months I m writing this . I faced no issues till now. Apollo staff was also very caring and good. I would mention Apollo Hospital, Navi Mumbai in specific. Good follow up diet makes it normal. I would strongly recommend Dr Nitish. He knows his job perfectly. He is not money minded at all. He would recommend surgery only if it’s required.
I was diagnosed with gall stones a year ago in Delhi, I showed it to a doctor at M.... hospital, he .... asked me to get a surgery done and get my gall removed on any date of my choice, I was sacred and too young to get it done I got a vibe from doctor that for him it’s just a small things, however according to for a patient it’s important first be convinced on the urgency to get it done and feel safe . A year later I shifted to Mumbai and started having a frequent pain in shoulder blades and gall area. It went sharp this time. We went to Dr Nitish , as oppose to Delhi doc, Dr Nitish was very polite, first asked us to get the scan done and understand the current scenario, the scan showed one big 17 mm stone which was earlier also there but this time also there were multiple various sized stones as well along with the big one. Dr Nitish examined the scan, explained me and my husband about the condition and need of surgery or else the stone Would have slipped in the panacea or bile calling for a bigger operation. He explained diagramatically . He was patient in explaining, gave us time to think and be convinced. We were ready and then he performed it . It was flawless, quick and went well. He is a very experienced and fine surgeon , he is caring and doesn’t create panic at all rather he takes it slowly and makes patient comfortable. It was lapro, it’s been 2 months I m writing this . I faced no issues till now. Fortis staff was also very caring and good. I would mention fortis Vashi in specific. Good follow up diet makes it normal. I would strongly recommend Dr Nitish. He knows his job perfectly. He is not money minded at all. He would recommend surgery only if it’s required.
I had surgery of my left hydrocele on 27th May 2017 by Dr Nitish Jhawar. An excellent experience of service I got particularly from Dr Jhawar. He is not only a qualified experienced doctor but also a splendid human being. Thanks a lot.
It was a Laparoscopic operation for the removal of Gall Bladder (stones). I had developed on and off pain in abdomen before the operation, after the operation feeling good, totally pain free. Thanks and respect for handling my case very well.
I met doctor Nitish for piles problem and wanted to undergo LASER procedure only, my operation is successful and I thank doctor for being a good human being and great surgeon.
I was suffering from piles since long time. For bleeding heavily I met Dr Nitish Jhawar and after meeting him decided to go for Stapler surgery for piles. I found him a doctor who listens to our problem and explains properly.
I got diagnosed about a year back but was avoiding operation for Hernia repair, Dr Nitish Jhawar explained me why surgery should be done and I chose surgery by laparoscopy method. I am happy with the doctor and the hospital.
I visited for Gall Bladder removal by Laparoscopy after searching for best laparoscopic surgeon. After meeting dr my fear for surgery was vanished and my surgery went well and recovery was smooth.
Honest doctor, expert in his field....can trust his words
Very good he describe everything in very pleasant manner about the problem which was very helpful to me to understand my disease.
Very nice. Doctor is very patient and gives you correct advice.
He is very erudite and smart at getting to the bottleneck of the problem. And before realized he had pinched away d growth bothering me near my anal area.
Dr. Jhawar is few of the best doctors in town. Extremely pleasant and comfortable experience